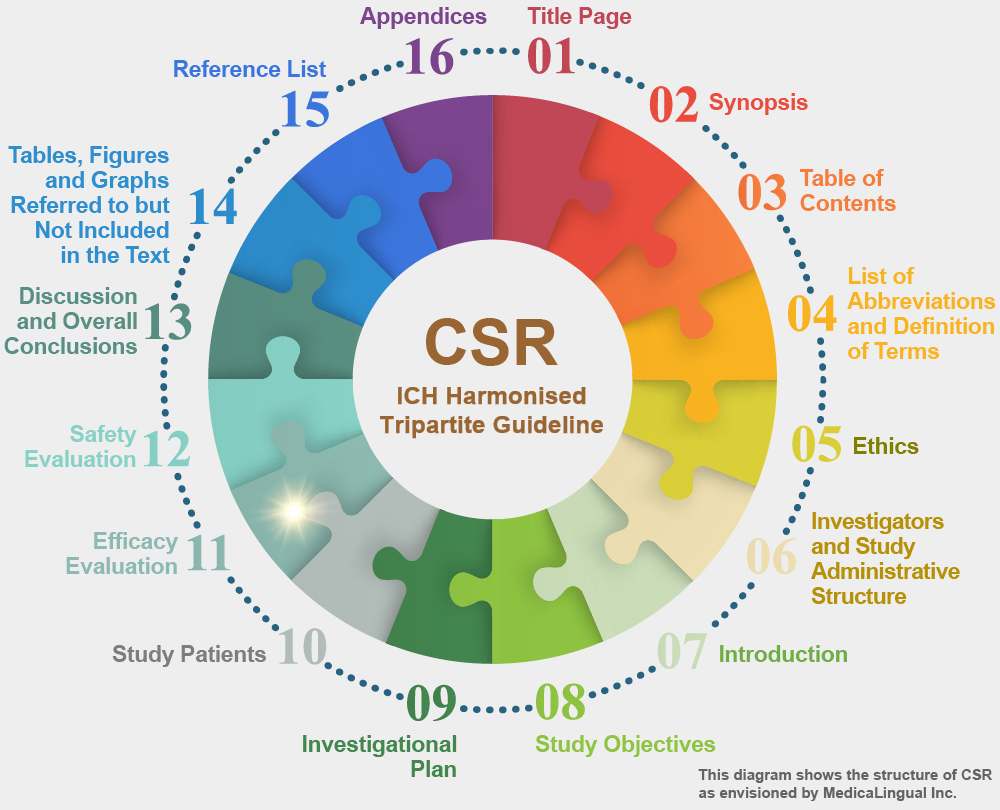
治験の統括報告書の構成と内容に関するガイドライン
平成8年5月1日 薬審第335号
各都道府県衛生主管部(局)長あて 厚生省薬務局審査課長通知
STRUCTURE AND CONTENT OF CLINICAL STUDY REPORTS
Recommended for Adoption at Step 4 of the ICH Process on 30 November 1995 by the ICH Steering Committee
11. 有効性の評価
11.4 有効性に関する成績及び個別患者データ一覧表
11.4.1 有効性の解析
主要な有効性の測定値全て(主たるエンドポイント及び副次的エンドポイント;調査された全ての薬力学的エンドポイント)について治療群間で比較すること。同様に,各患者におけるリスク・ベネフィットの評価が行われていれば,それらについても比較すること。一般に,有効性の検証を目的とした試験では,治験実施計画書で計画した解析の結果及び治験中のデータのある患者を全て含めた解析の結果を示すこと。その解析では,治療間の差の大きさ(点推定)及びそれに伴う信頼区間を示すこと。また,仮説検定を実施したならば,その結果も示すこと。
11. EFFICACY EVALUATION
11.4 EFFICACY RESULTS AND TABULATIONS OF INDIVIDUAL PATIENT DATA
11.4.1 ANALYSIS OF EFFICACY
Treatment groups should be compared for all critical measures of efficacy (primary and secondary end-points; any pharmacodynamic end points studied), as well as benefit/risk assessment(s) in each patient where these are utilised. In general, the results of all analyses contemplated in the protocol and an analysis including all patients with on-study data should be performed in studies intended to establish efficacy. The analysis should show the size (point estimate) of the difference between the treatments, the associated confidence interval, and where utilised, the results of hypothesis testing.
連続変数(例えば,平均血圧,抑うつ尺度評点)に基づく解析も,反応による分類(例えば,感染症の治癒)に基づく解析も,ともに妥当であり得る。両方ともに計画されており,実施されたならば,両方とも提示すること。もし,(統計解析計画にはない)新しい分類を作った場合には,それらの根拠について説明すること。たとえ一つの変数(例えば,血圧試験における×週目の臥位血圧)に主たる関心があるとしても,他の適切な測定値(例えば,立位血圧や他の特定の時点での血圧)についても少なくとも簡潔に評価すること。さらに,可能な限り反応の時間的経過を記述すること。多施設共同治験においては,適切であれば特に症例数の多い施設に関して,重要な変数についての施設ごとのデータの表示と解析を含めることにより,個々の施設の結果を正確に描写すること。
Analyses based on continuous variables (e.g., mean blood pressure or depression scale score) and categorical responses (e.g., cure of an infection) can be equally valid; ordinarily both should be presented if both were planned and are available. If categories are newly created, (i.e., not in the statistical plan) the basis for them should be explained. Even if one variable receives primary attention (e.g., in a blood pressure study, supine blood pressure at week x), other reasonable measures (e.g., standing blood pressure and blood pressures at other particular times) should be assessed, at least briefly. In addition, the time course of response should be described, if possible. For a multicentre study, where appropriate, data display and analysis of individual centres should be included for critical variables to give a clear picture of the results at each site, especially the larger sites.
有効性又は安全性の転帰について,主要な測定又は評価が複数のグループでなされた場合には(例えば,ある患者が急性心筋梗塞であったかどうかについて,治験責任医師と専門家委員会の双方から意見が出されるような場合),それらの評価間の全体的な差を示し,個々のどの患者が異なった評価を受けたかを明らかにすること。全ての解析においてどの評価を用いたかを明らかにすること。
If any critical measurements or assessments of efficacy or safety outcomes were made by more than one party (e.g., both the investigator and an expert committee may offer an opinion on whether a patient had an acute infarction), overall differences between the ratings should be shown, and each patient having disparate assessments should be identified. The assessments used should be clear in all analyses.
多くの場合,有効性と安全性のエンドポイントを区別する(例えば,致死性の疾患の治験における死亡など)ことは難しい。以下に示した原則の多くを主要な安全性の評価項目においても適用すること。
In many cases, efficacy and safety endpoints are difficult to distinguish, (e.g., deaths in a fatal disease study). Many of the principles addressed below should be adopted for critical safety measures as well.
ガイドライン ― Q&A
統計的推定の重視
Q12:「11.4.1有効性の解析」において信頼区間の記述が求められているが?
A12:統計的検定だけではなく,推定に重点がおかれていることが本ガイドラインの特徴の一つである。ガイドライン本文に「主要な有効性の測定値全てについて治療群間で比較すること」とあるが,その際は,点推定値(例えば,有効率,平均値など)とその信頼区間を示し,さらに検定を実施した場合には,検定結果(p 値等)も併せて示していただきたい。すなわち,検定の結果としてのp 値だけではなく,要約統計量や基礎的な統計量の記述を要求していることが重要である。
***