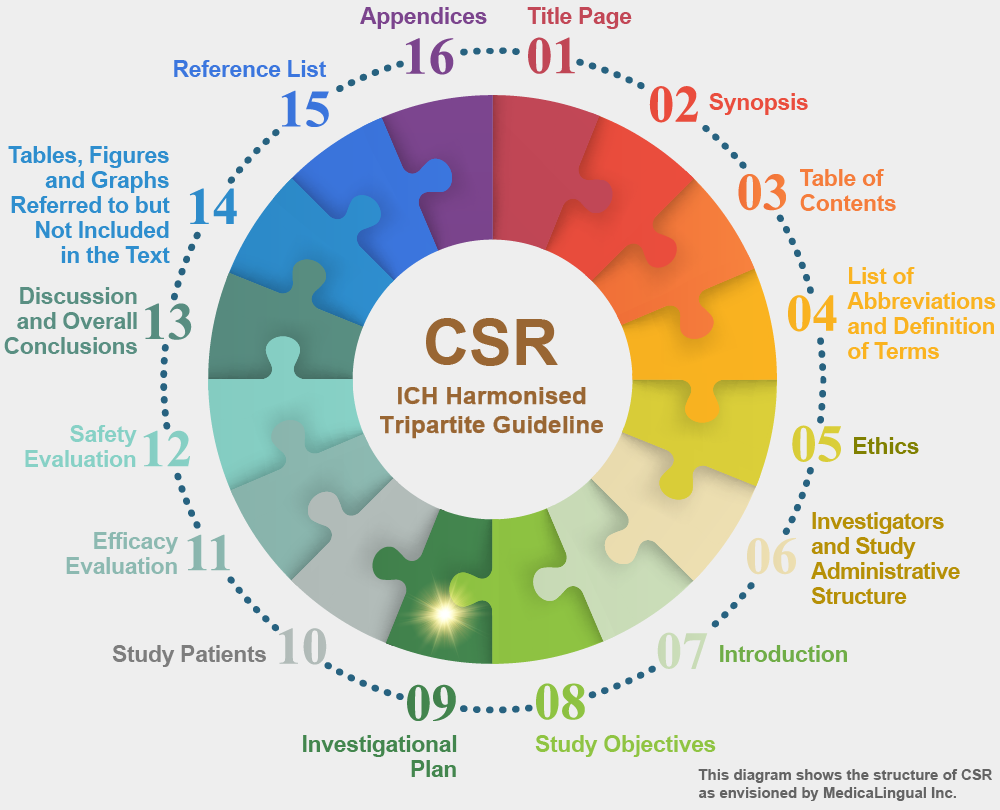
治験の統括報告書の構成と内容に関するガイドライン
平成8年5月1日 薬審第335号
各都道府県衛生主管部(局)長あて 厚生省薬務局審査課長通知
STRUCTURE AND CONTENT OF CLINICAL STUDY REPORTS
Recommended for Adoption at Step 4 of the ICH Process on 30 November 1995 by the ICH Steering Committee
9. 治験の計画
9.3 治験対象集団の選択
9.3.1 組み入れ基準
患者母集団及び患者を治験に組み入れるために用いた選択基準を記述し,治験の目的に照らしてその母集団が適切であることを考察すること。
9. INVESTIGATIONAL PLAN
9.3 SELECTION OF STUDY POPULATION
9.3.1 INCLUSION CRITERIA
The patient population and the selection criteria used to enter the patients into the study should be described, and the suitability of the population for the purposes of the study discussed.
用いられた特定の診断基準及び疾患に要求される特定の事項(例えば,特定の重症度又は罹病期間,特定の検査,評価尺度若しくは身体的検査の結果,前治療が有効とか無効というような特定の病歴上の特徴,又は予後因子である可能性のある他の因子及び年齢,性別若しくは人種的因子)を提示すること。
Specific diagnostic criteria used, as well as specific disease requirements (e.g., disease of a particular severity or duration, results of a particular test or rating scale(s) or physical examination, particular features of clinical history, such as failure or success on prior therapy, or other potential prognostic factors and any age, sex or ethnic factors) should be presented.
スクリーニングの基準及び無作為化時又は治験薬による治療への組み入れ時に判断するための追加基準について記述すること。治験実施計画書では定義されていない付加的な組み入れ基準があったと考えられる理由がある場合には,それらの意味合いについて考察すること。例えば,治験責任医師によっては,特定の病態又は特定の初期状態を有する患者を除外したり,他の試験に組み入れたりしたかもしれない。
Screening criteria and any additional criteria for randomisation or entry into the test drug/investigational product treatment part of the trial should be described. If there is reason to believe that there were additional entry criteria, not defined in the protocol, the implications of these should be discussed. For example, some investigators may have excluded, or entered into other studies, patients who were particularly ill or who had particular baseline characteristics.
9.3.2 除外基準
治験への組み入れ時点での除外基準を特定し,その根拠(例えば,安全性への配慮,管理上の理由又は治験対象としての適切性の不足)を示すこと。試験結果を一般化する際の除外の影響について,報告書13章又は安全性及び有効性の総括的な分析のなかで考察すること。
9.3.2 EXCLUSION CRITERIA
The criteria for exclusion at entry into the study should be specified and the rationale (e.g., safety concerns, administrative reasons or lack of suitability for the trial) provided. The impact of exclusions on the generalisability of the study should be discussed in section 13 of the study report, or in an overview of safety and efficacy.
9.3.3 患者の治療又は評価の打ち切り
患者の治療又は評価観察を打ち切る理由があらかじめ定められていれば記述し,さらにそれらの患者についての追跡観察の種類と期間が計画されていれば記述すること。
9.3.3 REMOVAL OF PATIENTS FROM THERAPY OR ASSESSMENT
The predetermined reasons for removing patients from therapy or assessment observation, if any, should be described, as should the nature and duration of any planned follow-up observations in those patients.
デザイン上の重要な特徴(患者の選択,治験のエンドポイント,期間,実対照薬の用量,併用療法など)が当該治験に類似しており,当該実対照薬がプラセボより優れているという結果を一貫して示す過去の試験成績を分析することで,裏付けが得られることもあろう。当該治験が,有効な治療と無効な治療とを区別する能力を持つことをどのように示せるのかについても考察すること。例えば,治療集団と無治療群を明確に区別する治療上の反応の大きさを(過去の試験成績に基づき)定めることができるかもしれない。このような反応は,基準値からの測定値の変化,又は治癒率若しくは生存率のような特定の転帰である場合もある。このような反応が達成されたならば,当該治験が活性を有しない薬剤と活性を有する薬剤とを識別し得たとの期待が支持されよう。その治験で,治療法が一定以上に劣らないことを示そうとした治療効果の差(しばしばデルタ値と言われる)についても考察すること。
Support may be provided by an analysis of previous studies similar to the present study with respect to important design characteristics (patient selection, study endpoints, duration, dose of active control, concomitant therapy etc.) showing a consistent ability to demonstrate superiority of the active control to placebo. How to assess the ability of the present study to distinguish effective from ineffective therapy should also be discussed. For example, it may be possible to identify a treatment response (based on past studies) that would clearly distinguish between the treated population and an untreated group. Such a response could be the change of a measure from baseline or some other specified outcome like healing rate or survival rate. Attainment of such a response would support the expectation that the study could have distinguished the active drug from an inactive drug. There should also be a discussion of the degree of inferiority of the therapy (often referred to as the delta value) the study was intended to show was not exceeded.
既存対照の限界はよく知られており(治療群の比較可能性の保証の困難さ,治療法に関して治験責任医師等に盲検化ができないこと,治療法や疾患の変化,プラセボ効果による差など),特別な注意が必要である。
The limitations of historical controls are well known (difficulty of assuring comparability of treated groups, inability to blind investigators to treatment, change in therapy/disease, difference due to placebo effect etc.) and deserve particular attention.
ウォッシュアウト期間の有無及び治療期間の長さを含む,デザインのその他の特徴についても考察する価値があろう。特に慢性疾患の場合にはその価値がある。もし,用量及び投与間隔を選択した理由が明白でないならば,それを合理的に説明すること。例えば,消失半減期の短い薬剤であって,作用が血中濃度の時間的推移に密接に関係している場合は,通常その薬剤を1日1回投与することでは有効性は示されない。もし,治験デザインがそういった投与法を用いているのであれば,例えば,血中濃度に比較して作用が持続するという薬力学的証拠を示すことによって説明すること。次の投与の直前には薬剤の作用が「消失している」という証拠を探索するために用いた手順,例えば投与直前の作用の測定のような手順を記述すること。同様に,並行デザインによる用量-反応試験においては,それらの用量が選択された理由を説明すること。
Other specific features of the design may also deserve discussion, including presence or absence of washout periods and the duration of the treatment period, especially for a chronic illness. The rationale for dose and dose-interval selection should be explained, if it is not obvious. For example, once daily dosing with a short half-life drug whose effect is closely related in time to blood level is not usually effective; if the study design uses such dosing, this should be explained, e.g., by pointing to pharmacodynamic evidence that effect is prolonged compared to blood levels. The procedures used to seek evidence of “escape” from drug effect at the end of the dose-interval, such as measurements of effect just prior to dosing, should be described. Similarly, in a parallel design dose-response study, the choice of doses should be explained.